
Naperville Integrated Wellness
NAPERVILLE'S TOP RATED LOCAL® FUNCTIONAL MEDICINE FACILITY

Motility Dysfunction: When Digestion Slows, Stalls, or Moves Too Fast
Digestive distress is often blamed on the wrong foods, but many persistent symptoms stem from something more fundamental: impaired movement within the gastrointestinal tract. Our motility dysfunction specialist in Naperville looks to the root of the problem with this disorder. When the gut loses its coordinated rhythm, issues like bloating, reflux, constipation, and diarrhea can persist regardless of diet, signaling a deeper breakdown in digestive regulation rather than a simple food reaction. Learn more from Dr. Sharon Borkowski on mobility dysfunction now!
Why Motility Matters More Than Most People Realize
Most people think digestion is about what they eat. In reality, it is equally about how well the gut moves.
Motility is the engine of digestion. Without coordinated movement, even the cleanest diet can create bloating, reflux, constipation, diarrhea, nausea, and persistent discomfort. You can remove gluten, eliminate dairy, avoid sugar, and still feel miserable if the mechanical process of digestion is impaired.
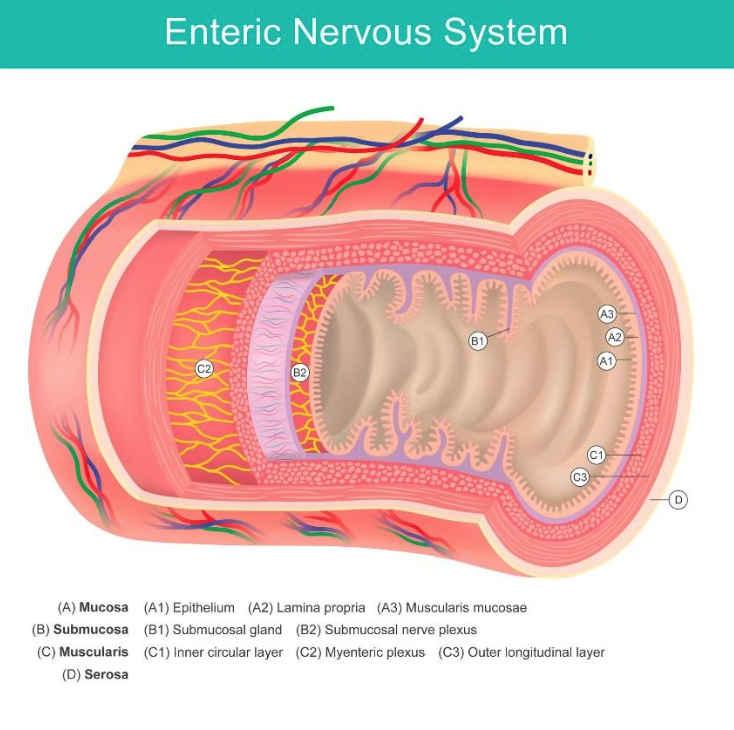
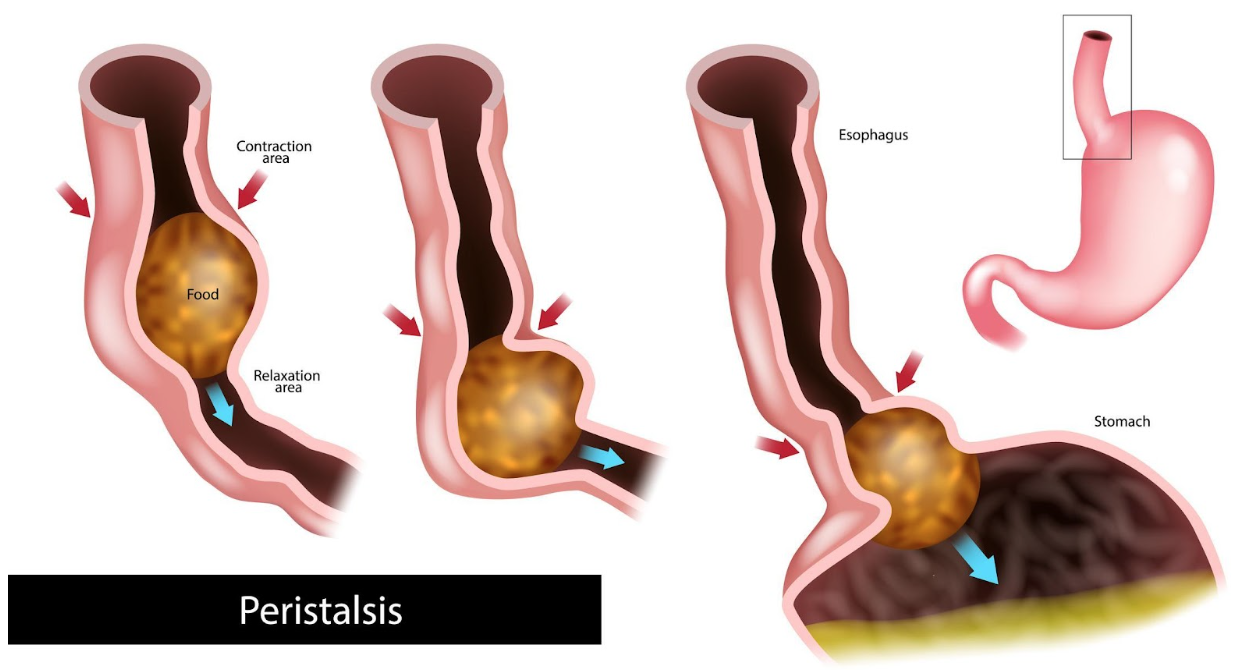
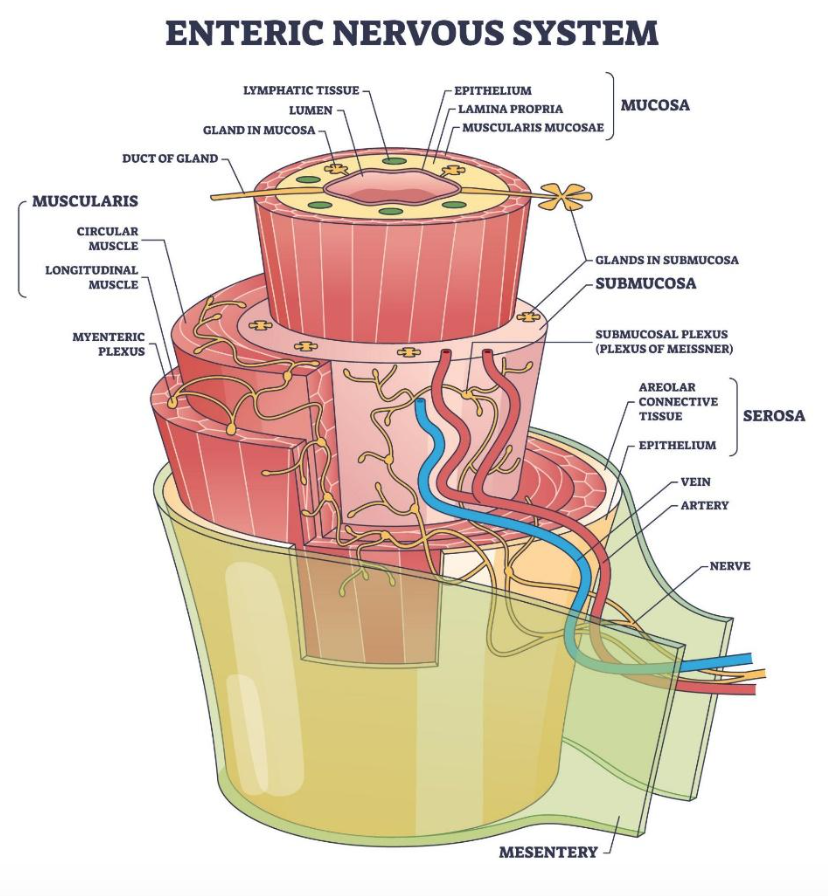
From a clinical perspective at Naperville Integrated Wellness, many patients presenting with chronic digestive symptoms are not reacting to food itself. They are experiencing dysfunction in the movement of the gastrointestinal tract. The system is not coordinating properly. Conventional care often focuses on suppressing symptoms: But rarely is the deeper question asked: Why isn’t the gut moving properly? At Naperville Integrated Wellness, we approach digestion differently. We evaluate the neurological, hormonal, inflammatory, immune, and metabolic drivers influencing motility. Because when movement fails, everything downstream begins to fail. Gastrointestinal motility refers to the coordinated muscular contractions that move food, fluids, bacteria, and waste through the digestive tract—from the esophagus all the way to the colon. This includes: The enteric nervous system contains millions of neurons embedded in the gut wall. It communicates constantly with the brain through the vagus nerve. When this communication is disrupted, coordination breaks down. Proper motility is not optional. It: When motility is disrupted, one of two things occurs: stagnation or acceleration. Both create dysfunction. Imbalanced gut motility—whether sluggish, accelerated, or erratic—disrupts digestion in different ways, from microbial overgrowth and inflammation to malabsorption and nutrient depletion. When these patterns fluctuate over time, it reflects impaired coordination within the digestive system rather than isolated symptoms, often pointing to an underlying regulatory dysfunction. When movement slows, symptoms may include: Food and waste linger too long. Fermentation increases. Gas accumulates. Inflammation rises. Over time, microbial imbalance can develop. Slow motility often feeds into conditions like small intestinal bacterial overgrowth (SIBO), creating a vicious cycle: stagnation promotes overgrowth, and overgrowth further slows movement. When movement is too rapid: Food passes through before digestive enzymes and bile can adequately break it down. Nutrient deficiencies may follow, even in individuals eating a nutrient-dense diet. This is common in IBS-mixed patterns. Symptoms fluctuate: Often this pattern emerges after infections, major stress events, antibiotic use, or inflammatory episodes. The gut’s coordination becomes erratic rather than simply slow or fast. Motility patterns can shift over time in chronic conditions. A patient may begin with constipation and later develop alternating symptoms. That evolution signals deeper dysfunction—not randomness. Motility issues often present subtly at first. Over time, they become more disruptive. Common symptoms include: Symptoms frequently intensify with: The gut does not function independently. It responds to systemic signals. Motility is influenced by the entire physiological environment. Motility problems rarely occur in isolation. They are downstream consequences. The migrating motor complex (MMC) — the “cleansing wave” of the small intestine — is highly dependent on vagal tone. When sympathetic dominance becomes chronic, digestive signaling is deprioritized in favor of survival pathways. Reduced parasympathetic activity weakens coordinated contractions, slows gastric emptying, and diminishes bowel propulsion. Patients often report bloating that worsens under stress, even when diet remains unchanged. Over time, impaired brain–gut communication alters sensitivity as well as movement, creating a pattern where stress alone can trigger constipation, urgency, or alternating bowel shifts. Inflammation interferes with smooth muscle performance and disrupts enteric nerve signaling. Even subtle, ongoing immune activation can blunt the precision of peristaltic waves. Cytokines released in inflamed tissue alter neurotransmitter balance in the gut wall, reducing coordinated contraction strength. This often manifests as incomplete evacuation, sluggish transit, or irregular stool patterns. If gut inflammation persists, structural and functional changes in the intestinal lining can further impair motility, creating a feedback loop between irritation and dysfunction. Acute gastroenteritis can trigger long-term changes in neuromuscular signaling. In some individuals, immune responses mistakenly target proteins involved in the migrating motor complex. This autoimmune-style disruption may reduce the strength or frequency of cleansing waves in the small intestine. As a result, food residue lingers longer than intended. Months or even years after the initial infection, patients may develop persistent bloating, altered stool patterns, or SIBO driven by this impaired motility foundation. Effective motility prevents excessive bacterial accumulation in the small intestine. When transit slows, microbes gain time and substrate to proliferate beyond their normal range. The gases produced — particularly methane — can directly inhibit smooth muscle activity, further reducing transit speed. Hydrogen-dominant overgrowth may instead accelerate movement in some cases. This bidirectional relationship means motility impairment both contributes to and results from microbial imbalance. Thyroid hormones regulate basal metabolic rate at the cellular level, including within intestinal smooth muscle. Hypothyroidism commonly presents with slowed transit and constipation. Cortisol fluctuations influence autonomic balance, shifting digestive tone toward inhibition when chronically elevated. Stress hormones alter both secretion and contraction patterns. Reproductive hormones also affect bowel rhythm. Progesterone tends to relax smooth muscle, while estrogen shifts can influence fluid dynamics in the colon, altering stool consistency and frequency. Smooth muscle contraction depends on adequate magnesium and calcium balance. Insufficient magnesium can impair both contraction and relaxation phases of peristalsis. B vitamins and iron are essential for mitochondrial energy production and nerve conductivity. Without sufficient cellular energy, coordinated waves weaken. Over time, malabsorption caused by motility dysfunction can worsen these deficiencies, compounding the underlying problem. Certain medications interfere with neurotransmitters responsible for gut contraction. Opioids suppress peristalsis by binding to receptors in the enteric nervous system. Anticholinergic agents blunt acetylcholine signaling, reducing contractile strength. Some antidepressants alter serotonin pathways that regulate bowel rhythm. Acid-suppressing medications may indirectly contribute by changing microbial patterns, which can then influence motility dynamics. Chronic hyperglycemia damages autonomic nerves, including those controlling digestive movement. This form of neuropathy can blunt gastric and intestinal signaling. Erratic blood glucose also destabilizes energy delivery to smooth muscle cells, weakening contraction efficiency. In advanced cases, patients may experience alternating patterns as nerve signaling becomes inconsistent rather than uniformly slow. Treating motility dysfunction symptomatically — with laxatives, antidiarrheals, or prokinetics alone — may temporarily shift movement, but without correcting upstream drivers, regulation rarely stabilizes long term. Sustainable improvement requires restoring coordinated signaling across the nervous, immune, endocrine, and microbial systems. Colonoscopy may appear normal. Yet function can still be impaired. IBS is frequently used as a descriptive label. It describes symptom clusters but does not explain why coordination has broken down. Laxatives and acid blockers may provide temporary relief but do not restore neuromuscular function. Over time, chronic motility dysfunction can contribute to: The longer dysfunction persists, the more layered the condition becomes. Evaluation goes beyond isolated symptoms. We assess: The entire digestive timeline matters — not just a single complaint. Individualized evaluation replaces protocol-based care. Motility dysfunction is rarely caused by one factor. It requires pattern recognition and strategic sequencing. Treatment may include: Healing motility takes strategy, sequencing, and patience. There is no shortcut. It depends on duration and underlying drivers. Early dysfunction often normalizes fully when stress, inflammation, and nutrient deficiencies are corrected. Long-standing cases may require long-term management. That is not failure. It is stabilization and functional restoration within physiological limits. The key difference: Symptom suppression manages discomfort. Early intervention improves outcomes significantly. Persistent symptoms are signals. Ignoring them allows progression. Healing requires: Quick fixes rarely produce durable outcomes. Sustainable improvement requires understanding why the system became dysregulated in the first place. Naperville Integrated Wellness is located in Naperville, but offers functional medicine for St. Charles, Aurora, Downers Grove and more! Motility is foundational to gut health and whole-body wellness. When the gut moves properly: At Naperville Integrated Wellness, the focus is not on silencing symptoms — it is on understanding why movement has changed. If you are living with chronic bloating, constipation, diarrhea, reflux, or unexplained digestive discomfort, it may not be the food (although it often plays a part). It may be the engine (Migrating Motor Complex of the Enteric Nervous System). Schedule a motility function specialist evaluation to begin identifying the root cause and restoring digestive coordination. Reach out to us at (630)210-8391 or and schedule your appointment today.
What Is Gastrointestinal Motility?
Types of Motility Dysfunction
Hypomotility (Slow Motility)
Hypermotility (Fast Motility)
Disorganized Motility
Common Symptoms of Motility Dysfunction
Root Causes of Motility Dysfunction (Functional Medicine Perspective)
Nervous System Dysregulation
Chronic Gut Inflammation
Post-Infectious Changes
Small Intestinal Bacterial Overgrowth (SIBO)
Hormonal Imbalances
Nutrient Deficiencies
Medications
Blood Sugar Dysregulation
Why Motility Disorders Are Often Missed
CT scans may appear normal.
Standard labs may appear normal.
How Functional Medicine Evaluates Motility
Functional Medicine and Natural Treatment Options For Motility
Can Motility Dysfunction Be Reversed?
Functional medicine aims to restore coordination.Who Should Seek Evaluation?
Living With Motility Dysfunction Near St. Charles
Schedule A Root-Cause Approach to Motility Disorders